MTHFR, Hashimoto’s, and Nutrients – Dr. Izabella Wentz
You may have heard of the term “MTHFR gene mutation” and may be wondering what it is. First, I’d like to say that I prefer the term “MTHFR gene variation” rather than “mutation.” The word mutation makes it sound like there’s something wrong with the person, while variation is more empowering – and in my opinion, also more accurate.
While the word “mutation” implies an occurrence that is rare, unnatural, or flawed, the MTHFR gene variation is common. In fact, it’s present in up to 55 percent of the European population, is naturally occurring, and often has no negative health consequences – unless expressed. [1]
I chose to use this terminology after learning that I was a carrier of two copies of the MTHFR gene. When I first saw my test results, I thought to myself, I have bad genes. I am flawed. I am broken. I am bad.
It’s quite easy to go down that path and feel victimized, and I don’t ever want you to feel victimized by knowing something about yourself.
The reason we do tests and learn about our genes is to feel empowered. While we can’t change our genes, I can tell you that we can absolutely change their expression! So if you have the MTHFR gene variation, or are thinking of testing for it, I hope that this overview empowers you.
In this article, you’ll learn about:
- Symptoms and diseases related to the MTHFR gene variation
- Genetic effects on nutrient extraction and common nutrient deficiencies
- How to test for the MTHFR gene variation and check your homocysteine levels
- How to support your methylation pathways with food and supplements
Understanding the MTHFR Gene Variation
It’s important to understand what it means to have the MTHFR gene variation, in order to determine if it may be contributing to some of the symptoms you’ve been experiencing.
The gene involved is the MTHFR (Methylenetetrahydrofolate Reductase) gene. This gene codes for the MTHFR enzyme, the enzyme that converts the amino acid homocysteine to methionine, a building block for proteins.
We receive two copies of the MTHFR gene from each parent. This means we may end up with two copies of the “normal” MTHFR gene, one “normal” copy and one copy with the genetic variant, or both copies with the genetic variant. I’ll expand a bit about two different genes that carry MTHFR variations, and I’ll break down the different test results and what they can mean, further down in the article.
Individuals with one or two copies of the genetic variation and low activity of the MTHFR enzyme may present with elevated homocysteine levels, which have been associated with inflammation, heart disease, pregnancy complications, and even miscarriages. [2] It has also been associated with higher rates of Down syndrome and birth defects in offspring of those with the MTHFR gene variation, as well as other issues that may manifest later on in life, such as an increased risk of blood clots and a higher risk of certain cancers. [3]
Mental health symptoms like brain fog, depression, irritability, and anxiety are related to impaired methylation. [4]
One of the key things to note is that this gene variation also prevents people from properly methylating, which is one of the body’s key detox processes that helps them get rid of toxins.
Methylation impairment can result in an impaired ability to clear out certain toxins such as mercury and arsenic, and may lead to multiple chemical sensitivities, as our detox system can become overwhelmed.
Furthermore, methylation issues can contribute to estrogen dominance, since excess estrogen must be eliminated through our detoxification system. [5] As all of these symptoms are all too common in Hashimoto’s, I designed a Liver Support Protocol to support the methylation pathways, back in 2015.
Studies have shown that another possible consequence of this gene variation includes being sensitive to certain anesthetics, such as nitrous oxide, which is commonly used for dental surgeries. [6] If you’re due for an operation and have the MTHFR gene variation, you can search for and print the following articles for your surgeon and anesthesiologist, to share this information with them and seek alternative anesthetic options:
There are also some odd symptoms of methylation issues that I have noticed in myself and clients, including heavy menstrual bleeding with large blood clots during one’s menstrual cycle (likely due to estrogen dominance), as well as a scaly “raw” and red rash under the nose.
For me personally, a proper dose of methylation support helped me eliminate the giant menstrual clots I used to have. The scaly red rash under my nose that my mom desperately tried to help me heal for years, vanished with methylation support as well.
I first started taking methylation support in 2013, and I attribute proper methylation support to my remission from Hashimoto’s symptoms.
I was intrigued when I came across a study of people with Down syndrome (who are known to have thyroid issues as they age), that suggested folate supplements helped with preventing thyroid issues. [7]
Interestingly, in 2020, I came off all of my supplements (including methylation-supportive ones) during the “lockdown”, as my support system virtually vanished overnight and I was providing 24/7 care to my toddler son, who was still waking up at night. During this time, my heavy menstrual bleeding, anxiety, and that awful under-the-nose rash, came back with a vengeance. After the world became a little more normal and I got back on my supplements, I was able to resolve these issues, but it took longer than I expected.
It’s not all doom and gloom, however. Dr. Ben Lynch (author of the book Dirty Genes) reports that those who are born with the MTHFR gene variation may also have some advantages, such as being more alert, productive, and focused.
As the owner of two MTHFR gene variations, I can surely attest to this!
Genetic Effects on Nutrient Extraction
The genetic variation can also play a role in vitamin deficiencies. Specifically, elevated homocysteine levels often caused by the MTHFR gene variation have been associated with nutrient deficiencies in vitamins B2, B6, B9 (folate), and B12. [8]
It may seem like common sense to take a supplement to address a deficiency in folate, but not all sources of vitamin B9 are created equally. While vitamin B9 can be found naturally in foods in the form of folate, it can also be found in the form of folic acid, a manufactured and synthetic version of folate that is present in most bargain-priced multivitamins, as well as often added to processed foods.
Unfortunately, synthetic folic acid can be highly problematic for individuals with the MTHFR gene variation, as they may have a difficult time processing this form of folate. Some professionals claim that this type of synthetic folate may even cause a build-up in the body, leading to toxicity.
Studies have shown that folic acid supplements can increase one’s risk of cancer, including prostate cancer — one more reason to ditch processed foods and your multivitamin. [9]
In my decade of studying the root causes of illness, I am often shocked by how well-meaning public health initiatives end up harming many individuals in an effort to help the masses. (I’m talking about you, fluoride programs, iodine fortification of salt, and of course, folic acid fortification!)
Correlation Between the Genetic Variation and Hashimoto’s
You may be wondering, “Does everyone with Hashimoto’s have this variation, and does it make Hashimoto’s worse?”
The answer is a bit complicated! A 2012 study by Arakawa and colleagues of thyroid patients with Hashimoto’s and Graves’, found that polymorphisms – that is, gene variations that may lead to the abnormal expressions – were as common in autoimmune thyroid disease as they were in the normal population. [10]
Additionally, the authors concluded that the severity of autoimmune thyroid disease (AITD) did not correlate with whether one had this gene variation or not.
Here’s an excerpt from the study:
Genotype and allele frequencies of the MTHFR +677C/T and +1298A/C polymorphisms showed no significant differences between healthy controls and patients with AITD; these genotype and allele frequencies did not influence the prognosis of AITD.
In other words, the likelihood of having one or both of the MTHFR polymorphisms, as well as the frequency of variants (alleles) of the MTHFR gene, were not found to be more prevalent in those who have autoimmune thyroid disease compared to those who do not.
But a 2020 study of 34 women with hypothyroidism actually found that the MTHFR gene variant is significantly associated with hypothyroidism. [11] Polymerase chain reaction-restriction fragment length polymorphism analyses were used for the genotyping of MTHFR polymorphisms. The results found that the MTHFR C677T variant was associated with hypothyroidism.
Furthermore, methylation issues may contribute to fertility issues in women with hypothyroidism. A 2020 study examined two cases of women with hypothyroidism and a history of infertility. [12] Even after optimizing TSH levels, one continued to experience miscarriages. However, after identifying that both of these women carried an MTHFR gene variation, and introducing a supplement that contains the methylated form of folate, zinc, vitamin B3, vitamin B6, vitamin B12, and cobalamin, both women were able to conceive and give birth to healthy babies.
Experimental studies have shown that methylation activity is lower in hypothyroidism, and higher in hyperthyroidism. [13]
In my opinion, methylation issues and the MTHFR gene variation can contribute to some of the symptoms commonly attributed to, or associated with, hypothyroidism; and proper methylation support is often a key to feeling your best with Hashimoto’s and hypothyroidism.
What is Homocysteine?
Homocysteine is a naturally occurring amino acid. [14] We need vitamins B2, B12, B6, and B9 (folate) to break down homocysteine, in order to convert it to methionine and cysteine. Methionine is an essential amino acid and antioxidant that synthesizes proteins, and cysteine is a nonessential amino acid that can help reduce inflammation and increase communication between immune cells.
High levels of homocysteine in the blood are believed to increase one’s risk of heart disease, stroke, Alzheimer’s disease, and osteoporosis. [15]
The MTHFR gene variation is associated with a buildup of homocysteine due to impaired methylation. The MTHFR gene produces an enzyme that helps regulate homocysteine levels in the body, and when this process is impaired due to a genetic variation, we can end up with higher levels of homocysteine. [16]
A deficiency in B vitamins can lead to higher homocysteine levels, so those with the MTHFR gene variation can support healthy levels by supplementing with methylated versions of folate, B6, and B12. Rootcology’s MTHFR Pathways is formulated specifically to facilitate the efficient metabolism of homocysteine. Speaking on the topic of fertility, elevated homocysteine levels have been associated with miscarriage. [17] Through August 11th, you can get this supplement that has helped thousands of my readers, for 10% off! Simply enter the code MTHFR2023 at checkout.

Testing for the MTHFR Gene and High Homocysteine Levels
You can take genetic tests to find out whether you have this gene, as well as high homocysteine levels.
It’s important to test for both homocysteine levels and the MTHFR gene variation because, while you may not have the gene that affects the methylation pathways, you may still have elevated homocysteine levels, which tells us the level of inflammation in our bodies. Elevated homocysteine levels may also indicate a deficiency in B vitamins, specifically B2, B6, B12 and folate. [18]
While higher levels of homocysteine have been associated with numerous health complications, levels of homocysteine that are too low can also be problematic and have been associated with peripheral neuropathy (often felt as hand and arm tingling) and an impaired ability to make glutathione, an important antioxidant that reduces inflammation in the body.
Low levels of glutathione have been correlated with Hashimoto’s and heavy metal toxicity. [19]
Testing for homocysteine levels is now available through many labs and can be assessed with a blood test.
There are differing parameters for what may be considered optimal reference ranges for homocysteine levels. Depending on the lab, some reference ranges may define homocysteine excess as greater than 10 or 11 µmol/L, and levels under 4, 5, or even 6 µmol/L may be considered too low.
Other reference ranges, such as the one reported by Medscape, break down homocysteine levels by age and gender. (Levels of homocysteine generally increase with age.)
- Age 0-30 years: 4.6-8.1 µmol/L
- Age 30-59 years: 6.3-11.2 µmol/L (males); 4.5-7.9 µmol/L (females)
- Age >59 years: 5.8-11.9 µmol/L
According to functional ranges, however, the optimal homocysteine levels range seems to be somewhere between 5-7 µmol/L. I imagine that, as with most labs, homocysteine levels are simply numbers to consider when looking at the big picture of overall health, and individual variations need to be considered.
As for testing for the MTHFR genetic variation, many labs also offer tests for this gene. For example, you can order a genetic saliva test kit from 23andme.com, or see if you can get a genetic test from your physician, which may be covered by insurance. You can upload your results to geneticgenie.org, which will then tell you if you have the genetic variation.
However, some may be concerned with this genetic information getting reported on insurance or to employers. There have been concerns that having the MTHFR variation or elevated homocysteine levels could potentially interfere with future insurance coverage, that may limit pre-existing conditions.
Fortunately, one can order confidential tests that will not be reported to insurance, by using online lab testing services, like the Ulta Labs test for homocysteine or the Ulta Labs MTHFR gene variation test.
There are two possible MTHFR variations that you may have. Both the 677 and 1298 genes can carry the MTHFR variations.
These are the different types of potential variations to look for:
- Homozygous variation – You have two copies of the same MTHFR variation (either two variations on 677 or 2 variations on 1298).
- Heterozygous variation – You have one copy of the MTHFR variation on either the 677 gene or the 1298 gene.
- Compound heterozygous variation – You have one normal 677 and 1298 gene, and one variation on both the 677 and 1298 genes.
Elevated homocysteine, whether you have or don’t have the MTHFR gene variation, can indicate inflammation in the body. While people with elevated homocysteine may benefit from dietary interventions and supplementation (especially if the elevation was caused by inflammatory foods and nutrient deficiencies), other reasons for inflammation should be investigated with your practitioner as well.
Clinically, I have seen that having the MTHFR variation doesn’t necessarily mean one is destined for a lot of health challenges and symptoms, and having a greater number of variations doesn’t always mean the person will have more symptoms. I personally have two copies of the MTHFR mutation and am alive and well (with some interventions), while others I have seen have just one copy of a mutated gene, and a lot of symptoms.
There are various factors that determine the expression of these genes, such as the interaction of other genes, lifestyle choices, and interventions. Thus, I always say that genes are not our destiny. That said, I think knowing our genes is helpful, as it can provide us with a roadmap of knowing which areas may need more attention to minimize our symptoms.
While no research yet shows a connection to Hashimoto’s, I wanted to make note that in some cases, individuals may have normal blood levels of folate, but the folate may not be getting to the brain due to autoimmune folate receptor antibodies (FRAs), which block the transport of folate into the cerebral spinal fluid (CSF). This condition is known as cerebral folate deficiency, and has been implicated as a reversible cause of autism. [20]
Symptoms like irritability, anxiety, poor sleep, gross motor problems or problems with coordination, tics, seizures, vision problems, developmental delay and/or slowing of typical development, and depression have been reported in those with FRAs – and while testing folate levels in the CSF is too invasive, a test for folate receptor antibodies is available.
Interestingly, in addition to proper supplementation support, another recommended treatment for cerebral folate deficiency is a dairy-free diet (something I advocate for in Hashimoto’s too), as mammalian milk is thought to contribute to folate receptor antibodies, and may block folate transport to the brain. [21] I am following this topic closely to see if it becomes more relevant for thyroid health, and will share accordingly.
Symptoms That May Be Associated with Under- or Over- Methylation
How can you tell that you may be experiencing impaired methylation? Here are some symptoms of undermethylation to look out for: [22]
- Elevated homocysteine levels
- Depression
- Irritability
- Anxiety
- Multiple miscarriages
- Multiple chemical sensitivities
- Sensitivity to anesthetics
- Red face that lasts after exercising
- Allergies
- Being prone to addiction
- High libido
- Obsessive-compulsive disorder (OCD)
- Low pain threshold
- Headaches/migraines
- Digestive problems (such as IBS)
- Brain fog (especially after protein-rich meals)
- Insomnia
- High estrogen levels/estrogen dominance
- Low energy/fatigue
- Muscle pain
- Low levels of neurotransmitters (dopamine, norepinephrine, and serotonin)
- Heavy menstrual periods with blood clots
- Flakey skin rash under your nose*
- Lowered immunity*
*Although I haven’t seen this in the research, it’s been an observation for me personally, as well as for a few clients, that difficulty fighting off viral infections as well as having a red rash under the nose, seems to correlate with poor methylation. I have found that methylation support seems to really help me with this.
Symptoms of undermethylation should improve if you follow my recommendations for methylation support below.
Although undermethylation is more common with the MTHFR gene, overmethylation may instead be the case for some. This can affect the thyroid and adrenals, as well as cause other health problems. Overmethylation can also occur if people start taking methylation support supplements that are too potent (see the precautions section below for more information on what to do if this happens).
Symptoms of overmethylation can include: [23]
- Restless legs/pacing
- Hyperactivity
- High pain tolerance
- Histamine intolerance
- Sleep disorders
- Panic disorders
- Paranoia
- Insomnia
- Low libido
- ADHD
- Low motivation
- Depression
- Anxiety
- High levels of neurotransmitters (dopamine, norepinephrine, and serotonin)
- A high copper to zinc ratio
Generally, undermethylation will result in symptoms more akin to depression and sluggishness, while overmethylation is usually linked to symptoms like hyperactivity and anxiety. But it’s not always easy to tell what is happening without testing.
This is why it’s important to follow the directions of a health professional, and to use supplements carefully.
Supporting the Methylation Pathways
Once you know that your methylation pathways are impaired (rather than in overdrive), there are many things you can do to gently support and optimize your methylation pathways, including changing your diet, addressing nutritional deficiencies, and using supplements.
Food as Medicine
First, I recommend eating a diet that will lower the overall inflammation in your body, such as the Root Cause Paleo diet. (The plan that I recommend doesn’t just eliminate processed foods, but it also focuses on a high intake of veggies.)
As for addressing high homocysteine levels, there are two main nutrient pathways for breaking down homocysteine. Nutrient deficiencies along either of the pathways may result in elevated homocysteine levels. [24]
One of the pathways involves the use of the B vitamins, while the other one uses trimethylglycine (betaine) to help with metabolizing homocysteine. The following nutrients may support methylation and homocysteine levels: [25]
- Riboflavin (B2) – Rich sources include lamb, eggs, liver, salmon, and mushrooms.
- Vitamin B6 – Rich sources include meats, beans, avocados, nuts, and seeds.
- Folate (B9) – You can find folate present in its activated form in real foods such as green leafy vegetables (spinach, collard greens, and romaine lettuce are some examples), asparagus, papaya, beans (especially lentils), avocados, brussels sprouts, nuts, seeds, and beets.
- Vitamin B12 – This is primarily found in meats, and may be lacking in vegan or vegetarian diets, leading to deficiency.
- Betaine AKA trimethylglycine – Betaine can be found in beets, whole grains like quinoa (which some individuals may not be able to eat), and spinach.
Interestingly, beets are a very common food eaten in Poland, and I have noticed that many of my relatives in Poland who likely have the MTHFR gene variation do not have many symptoms.
Supplements to Support Methylation
Of course, we may not be able to get enough of the needed nutrients from food alone.
Individuals with the MTHFR gene variation and high homocysteine levels may also benefit from B2 (riboflavin), as well as activated versions of folate, B6, and B12, such as methylated folate (also known as L-5-MTHF Folate, methylfolate, 5-formyltetrahydrofolate or NatureFolate), Pyridoxal-5-Phosphate (P5P), and methylcobalamin, respectively.
In my survey of 2232 patients with Hashimoto’s, 45 percent of participants said they felt better after adding methylation-supporting supplements like methylated folate, B12, and B6 to their regimen.
Another 59 percent reported feeling better with adding the digestive enzyme betaine with pepsin as well, and I suspect this may in part be due to improved methylation. The top symptoms that improved included energy, pain, and mood.
Thus, if you also happen to have low stomach acid (as many people with Hashimoto’s do), taking the protein digestive enzyme Betaine with Pepsin from Rootcology is another great way to get extra trimethylglycine. Betaine HCl and pepsin are necessary for adequate absorption of vitamin B12, as well as protein, calcium, and iron.
I developed the Rootcology MTHFR Pathways supplement, which includes betaine and B12, to contain synergistic nutrients that support homocysteine pathways, including activated forms of folate, B2, and B6. And until August 11th at 11:59pm PT, you can get this supplement that has helped thousands of my readers for 10% off! Simply enter the code MTHFR2023 at checkout.
Please note: Rootcology currently ships to the United States only.
This combination may help to facilitate the efficient metabolism of homocysteine and maintain a healthy homocysteine pathway, allowing for the normal production of its necessary and important end products, including the sulfur-containing amino acids taurine and cysteine, and the neurotransmitters norepinephrine and dopamine.
An optimally functioning homocysteine pathway provides methyl and sulfur groups for biochemical reactions such as detoxification, healthy immune function, ideal joint and cartilage structure, and brain and cardiovascular health – so it’s important to metabolize homocysteine effectively. [26]
While some supplements for MTHFR focus mostly on using methylfolate, I wanted to add the additional ingredients, as they work in synergy.
Riboflavin, specifically, is often an overlooked component of a healthy methylation pathway and may help with migraines, fatigue, and lowering homocysteine levels in my experience. [27] Also known as vitamin B2, riboflavin is a critical cofactor for the methylation cycle, and ensuring proper levels can help optimize methylation.
I recommend supplementing as follows, based on your homocysteine level test results:
| Homocysteine Test Results | Number of Capsules per Day |
| <6 µmol/L | 1 |
| 6-9 µmol/L | 2 |
| 9-15 µmol/L | 3 |
| >15 µmol/L | 5 |
And if you’re looking for a better multivitamin, I recommend Nutrient 950 by Pure Encapsulations, which contains the active and methylated version of folate.
In addition, many of the lifestyle interventions helpful for Hashimoto’s are also beneficial for the MTHFR variation. I discuss these interventions in more detail in my first book, Hashimoto’s: The Root Cause, as well as in my second book, Hashimoto’s Protocol.
Precautions While Taking MTHFR Pathways
While most people with Hashimoto’s tend to feel better, about eight percent of people will feel worse with MTHFR Pathways. Some individuals may feel anxious if they start high-dose methylation support too quickly. Some of the people who feel slightly worse (i.e. those who may experience more anxiety and irritability) may benefit from a dosage reduction, in the case that their pathways are moving too quickly.
However, if “feeling worse” lasts more than a few days, this could be due to overmethylation, other gene variations such as an expressed CBS gene variation that may need to be supported before adding methylation support, or a sensitivity to the supplements, and the supplements should be discontinued.
In the case that you are overmethylating, yet are still deficient in folate and B12, you may want to avoid methylated versions of folate (methylfolate) and B12 (methylcobalamin), and consider non-methylated but active versions of folate (folinic acid) and B12 (adenosylcobalamin and/or hydroxocobalamin). I like Seeking Health’s Folinic Acid capsules and Pure Encapsulations’ Adenosyl/Hydroxy B12 drops.
As always, listen to your body and to your knowledgeable practitioners.
MTHFR Pathways should not be used with Addison’s disease, a history of electrolyte imbalance, diuretics, blood thinners, or steroid medications. As it contains a sulfur-based amino acid, it should also be avoided by those with sulfur sensitivity.
Other Nutrients That Can Help Symptoms
Curious about other nutrient deficiencies that may be the root cause of your symptoms, and supplements that may help address them? Download my free Supplements to Subdue Symptoms eBook to discover which supplements benefit which symptoms, and more!
The Takeaway
Some people have a genetic variation that may impair their detox abilities, affect how they absorb certain B vitamins, and contribute to their symptoms. Nonetheless, knowledge leads to empowerment. Again, while we can’t change our genes, we can absolutely change their expression!
You can support your methylation pathways with dietary interventions and supplements. To kickstart your path to wellness, I recommend testing your homocysteine levels and checking to see if you have markers for the MTHFR gene variation. If you do, supporting your methylation pathways with supplements may help reduce some of the symptoms you’re experiencing.
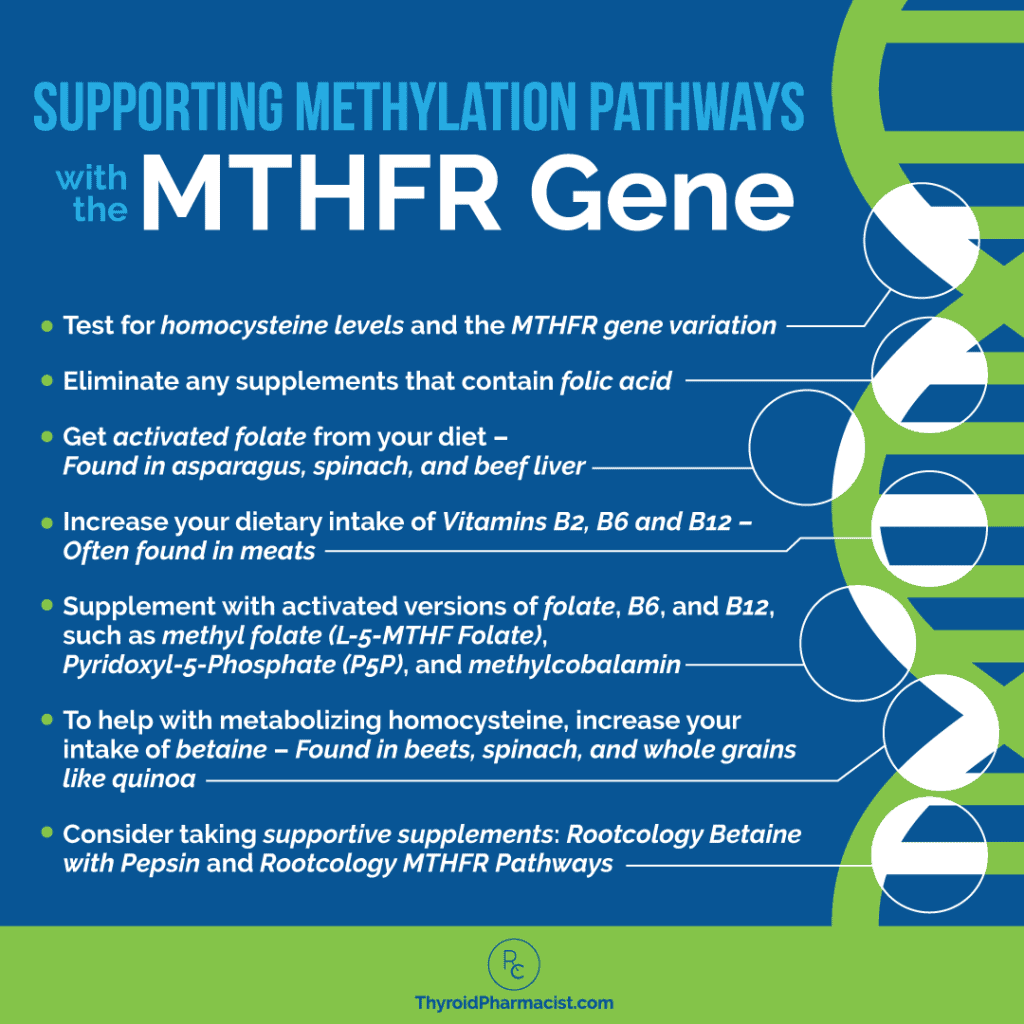
I’ve created a graphic to help you remember how to support your methylation pathways:
And of course, I’d like to reiterate this:
Share it on Facebook to remind yourself daily that knowledge about our bodies and our health EMPOWERS us and gets us one step closer to feeling our BEST!
I hope that this information empowers you, and I wish you all the best on your healing journey!
P.S. You can download a free Thyroid Diet Guide, 10 thyroid-friendly recipes, and the Nutrient Depletions and Digestion chapter of my first book for free by signing up for my newsletter. You will also receive occasional updates about new research, resources, giveaways, and helpful information.
For future updates, make sure to follow us on Facebook, Instagram, TikTok, and Pinterest!
References
[1] Yang B, Liu Y, Li Y, et al. Geographical distribution of MTHFR C677T, A1298C and MTRR A66G gene polymorphisms in China: findings from 15357 adults of Han nationality. PLoS One. 2013;8(3):e57917. doi:10.1371/journal.pone.0057917
[2] Son P, Lewis L. Hyperhomocysteinemia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; May 8, 2022.
[3] O’Leary VB, Parle-McDermott A, Molloy AM, et al. MTRR and MTHFR polymorphism: link to Down syndrome?. Am J Med Genet. 2002;107(2):151-155. doi:10.1002/ajmg.10121; Shi H, Yang S, Lin N, et al. Study on Maternal SNPs of MTHFR Gene and HCY Level Related to Congenital Heart Diseases. Pediatr Cardiol. 2021;42(1):42-46. doi:10.1007/s00246-020-02449-1; Liew SC, Gupta ED. Methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism: epidemiology, metabolism and the associated diseases. Eur J Med Genet. 2015;58(1):1-10. doi:10.1016/j.ejmg.2014.10.004
[4] Liew SC, Gupta ED. Methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism: epidemiology, metabolism and the associated diseases. Eur J Med Genet. 2015;58(1):1-10. doi:10.1016/j.ejmg.2014.10.004
[5] Födinger M, Hörl WH, Sunder-Plassmann G. Molecular biology of 5,10-methylenetetrahydrofolate reductase. J Nephrol. 2000;13(1):20-33.
[6] Nagele P, Zeugswetter B, Wiener C, et al. Influence of methylenetetrahydrofolate reductase gene polymorphisms on homocysteine concentrations after nitrous oxide anesthesia. Anesthesiology. 2008;109(1):36-43. doi:10.1097/ALN.0b013e318178820b; Nagele P, Brown F, Francis A, et al. Influence of nitrous oxide anesthesia, B-vitamins, and MTHFR gene polymorphisms on perioperative cardiac events: the vitamins in nitrous oxide (VINO) randomized trial. Anesthesiology. 2013;119(1):19-28. doi:10.1097/ALN.0b013e31829761e3
[7] Peeters, MA, Lejeune, J. Elevated TSH levels in young children with Down syndrome: Beneficial effects of supplemental folic acid. Ped Rev & Commns.1994; 8: 97-103.
[8] Son P, Lewis L. Hyperhomocysteinemia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; May 8, 2022.
[9] Figueiredo JC, Grau MV, Haile RW, et al. Folic acid and risk of prostate cancer: results from a randomized clinical trial. J Natl Cancer Inst. 2009;101(6):432-435. doi:10.1093/jnci/djp019; Ebbing M, Bønaa KH, Nygård O, et al. Cancer incidence and mortality after treatment with folic acid and vitamin B12. JAMA. 2009;302(19):2119-2126. doi:10.1001/jama.2009.1622
[10] Arakawa Y, Watanabe M, Inoue N, et al. Association of polymorphisms in DNMT1, DNMT3A, DNMT3B, MTHFR and MTRR genes with global DNA methylation levels and prognosis of autoimmune thyroid disease. Clinical and Experimental Immunology. 2012;170(2):194–201. doi:10.1111/j.1365-2249.2012.04646.
[11] Kvaratskhelia T, Abzianidze E, Asatiani K, Kvintradze M, Surmava S, Kvaratskhelia E. Methylenetetrahydrofolate Reductase (MTHFR) C677T and A1298C Polymorphisms in Georgian Females with Hypothyroidism. Glob Med Genet. 2020;7(2):47-50. doi:10.1055/s-0040-1714091
[12] Allam MM, El-Zawawy HT, Barakat SS, Ahmed SM, Saleh RNM. A hidden cause of infertility in hypothyroid patients. Clin Case Rep. 2020;8(2):374-378. Published 2020 Jan 14. doi:10.1002/ccr3.2654
[13] Lien EA, Nedrebø BG, Varhaug JE, Nygård O, Aakvaag A, Ueland PM. Plasma total homocysteine levels during short-term iatrogenic hypothyroidism. J Clin Endocrinol Metab. 2000;85(3):1049-1053. doi:10.1210/jcem.85.3.6439
[14] Homocysteine: Levels, tests, high homocysteine levels. Cleveland Clinic. May 7, 2021. Accessed July 6, 2023. https://my.clevelandclinic.org/health/articles/21527-homocysteine.
[15] Maron BA, Loscalzo J. The treatment of hyperhomocysteinemia. Annu Rev Med. 2009;60:39-54. doi:10.1146/annurev.med.60.041807.123308
[16] Varga EA, Sturm AC, Misita CP, Moll S. Cardiology patient pages. Homocysteine and MTHFR mutations: relation to thrombosis and coronary artery disease. Circulation. 2005;111(19):e289-e293. doi:10.1161/01.CIR.0000165142.37711.E7
[17] Nelen WL, Blom HJ, Steegers EA, den Heijer M, Thomas CM, Eskes TK. Homocysteine and folate levels as risk factors for recurrent early pregnancy loss. Obstet Gynecol. 2000;95(4):519-524. doi:10.1016/s0029-7844(99)00610-9
[18] Gilfix BM. Vitamin B12 and homocysteine. CMAJ. 2005;173(11):1360. doi:10.1503/cmaj.1050170
[19] Błażewicz A, Wiśniewska P, Skórzyńska-Dziduszko K. Selected Essential and Toxic Chemical Elements in Hypothyroidism-A Literature Review (2001-2021). Int J Mol Sci. 2021;22(18):10147. Published 2021 Sep 20. doi:10.3390/ijms221810147
[20] Cerebral folate deficiency in autism. The Autism Community in Action. Accessed July 6, 2023. https://tacanow.org/family-resources/cerebral-folate-deficiency/.
[21] Ramaekers VT, Sequeira JM, Blau N, Quadros EV. A milk-free diet downregulates folate receptor autoimmunity in cerebral folate deficiency syndrome. Dev Med Child Neurol. 2008;50(5):346-352. doi:10.1111/j.1469-8749.2008.02053.x; Berrocal-Zaragoza MI, Murphy MM, Ceruelo S, Quadros EV, Sequeira JM, Fernandez-Ballart JD. High milk consumers have an increased risk of folate receptor blocking autoantibody production but this does not affect folate status in Spanish men and women. J Nutr. 2009;139(5):1037-1041. doi:10.3945/jn.108.102475; Frye RE, Sequeira JM, Quadros EV, James SJ, Rossignol DA. Cerebral folate receptor autoantibodies in autism spectrum disorder. Mol Psychiatry. 2013;18(3):369-381. doi:10.1038/mp.2011.175
[22] Common symptoms of undermethylation or histadelia. Mensah Medical. http://www.mensahmedical.com/common-symptoms-of-undermethylation/. Published January 12, 2016. Accessed December 30, 2022.; 7 Signs You Need Methylation Support. https://education.seekinghealth.com/7-signs-you-need-methylation-support/. Accessed 7 January, 2022.
[23] A Look at Overmethylation. Designs for Health. Dec 6, 2018. https://blog.designsforhealth.com/node /910. Accessed 7 January 2022
[24] Homocysteine: Levels, tests, high homocysteine levels. Cleveland Clinic. https://my.clevelandclinic.org/health/articles/21527-homocysteine. Published May 7, 2021. Accessed December 30, 2022.
[25] Mahmoud AM, Ali MM. Methyl Donor Micronutrients that Modify DNA Methylation and Cancer Outcome. Nutrients. 2019;11(3):608. Published 2019 Mar 13. doi:10.3390/nu11030608
[26] Finkelstein JD. The metabolism of homocysteine: pathways and regulation. Eur J Pediatr. 1998;157 Suppl 2:S40-S44. doi:10.1007/pl00014300
[27] McNulty H, Dowey le RC, Strain JJ, et al. Riboflavin lowers homocysteine in individuals homozygous for the MTHFR 677C->T polymorphism. Circulation. 2006;113(1):74-80. doi:10.1161/CIRCULATIONAHA. 105.580332; García-Minguillán CJ, Fernandez-Ballart JD, Ceruelo S, et al. Riboflavin status modifies the effects of methylenetetrahydrofolate reductase (MTHFR) and methionine synthase reductase (MTRR) polymorphisms on homocysteine. Genes Nutr. 2014;9(6):435. doi:10.1007/s12263-014-0435-1
Note: Originally published in May 2015, this article has been revised and updated for accuracy and thoroughness.


