Positioning to take risk in two-sided contracts
by Joe Maher, CPA, MBA
Many health systems have intentionally delayed taking downside risk in payment contracting for many reasons. In some cases, organizations aren’t ready to perform in these contracts. In too many cases, there’s a detrimental level of risk aversion that’s impeding health systems from margin growth, particularly in value-based care (VBC) arrangements. Health systems and provider organizations that succeed in these contracts apply a sophisticated view of risk rather than as a binary.
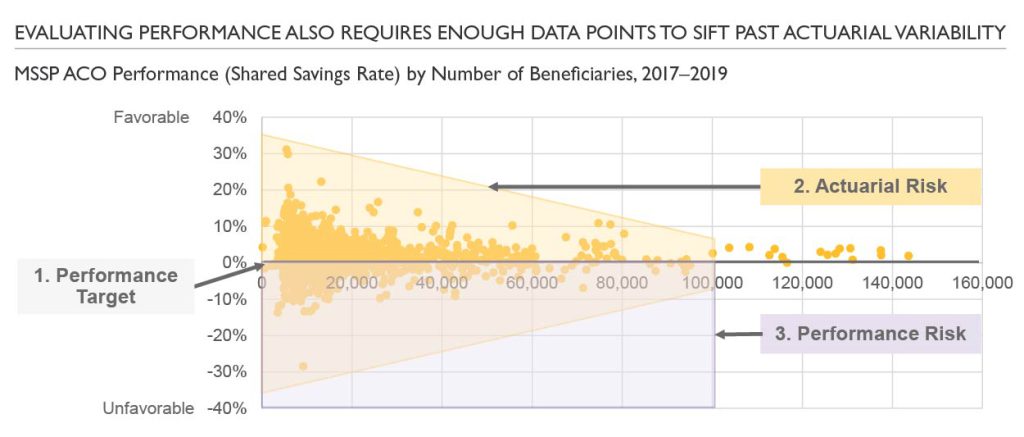
Moving more confidently into two-sided arrangements requires an understanding of the crucial components of risk in these contracts. Three key dimensions in establishing a two-sided contract are (1) the baseline performance target, (2) actuarial risk and (3) performance risk. Health systems that enter into contracting discussions with a strong understanding of these components are better positioned to evaluate and negotiate arrangements that can position the organization for success.
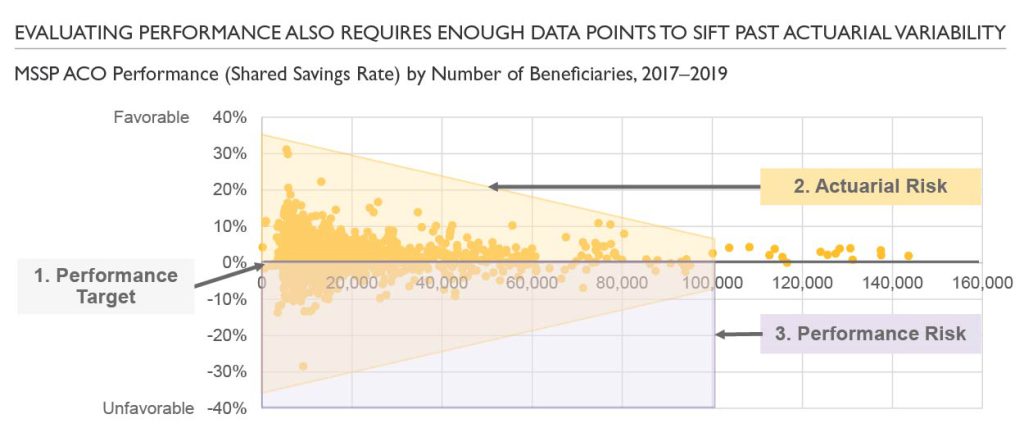
1. Baseline performance target: Establishing a reasonable and appropriate target is critical. For Medicare and Medicare Advantage (MA), risk score is an essential mechanism for ensuring the target fits the population. Regional benchmarks and historical performance are important inputs as well. Looking ahead, CMS is continuing to review model feedback to improve fairness and appropriateness of targets for risk-bearing organizations. This includes a transition to administrative benchmarking as well as a built-in growth rate component.
For commercial contracts establishing the baseline target often requires more involvement, in part because of less transparency between health plans and provider organizations. Rather than using a percent of the allocated premium dollar, these targets are based on historical performance, usually 1–3 years for a book of business. Additionally, agreed upon trend and modified risk adjustment methodologies (e.g., age, gender, industry) are important to allow the contract to evolve and avoid the ‘race to the bottom’ concern. Many provider organizations are concerned that continuous improvement will drive down the target, thus reducing their ability to capture shared savings.
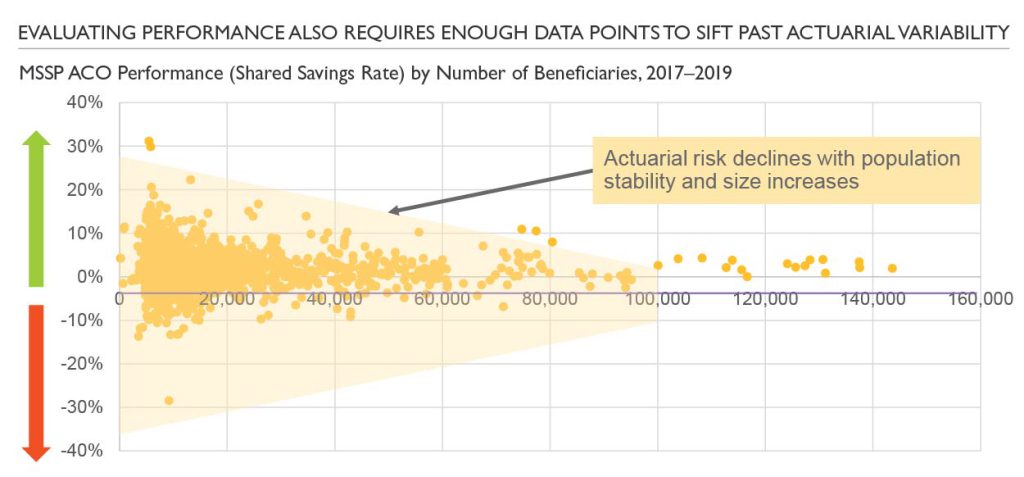
2. Actuarial risk: Managing populations entails inherent variability, especially with smaller group sizes. As group sizes increase, this risk usually declines. Additionally, these contracts should evaluate population stability as more stable populations with less turnover bring lower actuarial risk. Whereas any group (especially in the employer insurance space) with high churn will have greater variability and higher actuarial risk.
For health systems moving into two-sided contracts, the contracting approach should account for population size and stability. Additionally, there are contracting mechanisms, including stop-loss coverage levels and risk corridors, that further protect against less predictable risk. This also highlights the importance of maintaining a portfolio level view to better decipher between signal and noise when evaluating performance across contracts.
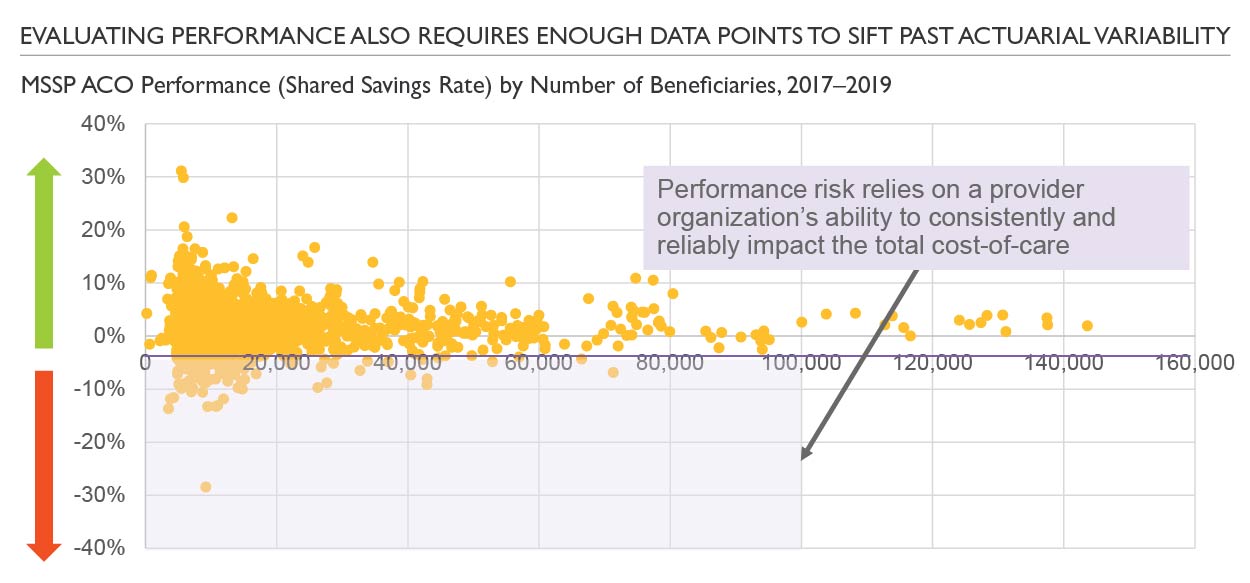
3. Performance risk: Managing populations entails inherent variability, especially with smaller group sizes. As group sizes increase, this risk usually declines. Additionally, these contracts should evaluate population stability as more stable populations with less turnover bring lower actuarial risk. Whereas any group (especially in the employer insurance space) with high churn will have greater variability and higher actuarial risk.
For health systems moving into two-sided contracts, the contracting approach should account for population size and stability. Additionally, there are contracting mechanisms, including stop-loss coverage levels and risk corridors, that further protect against less predictable risk. This also highlights the importance of maintaining a portfolio level view to better decipher between signal and noise when evaluating performance across contracts.
The playbook used by many of these organizations, including health plan delivery arms and VBC-focused providers, is to prioritize a high touch primary care-centric delivery model. This allows provider organizations to engage patients in the ambulatory setting with a technology-enabled care team that’s focused on improving their health and reducing their need for high-cost services (e.g., emergency department visits, hospitalizations and skilled nursing).
Readiness to take downside risk is important because two-sided contracts can be a strategic lever for amplifying upside. For example, let’s compare performance for a 25,000 life Medicare Accountable Care Organization (ACO) in two different risk-bearing models. This ACO could choose between the Direct Contracting model (DCE) with full risk and the Medicare Shared Savings Program (MSSP) with limited upside only. In this simplified example, the cumulative performance gains that accrued to this the entity taking on downside can be multiple times higher, with the following graph illustrating this performance comparison based on an annual estimated savings rate of about 2.0%.
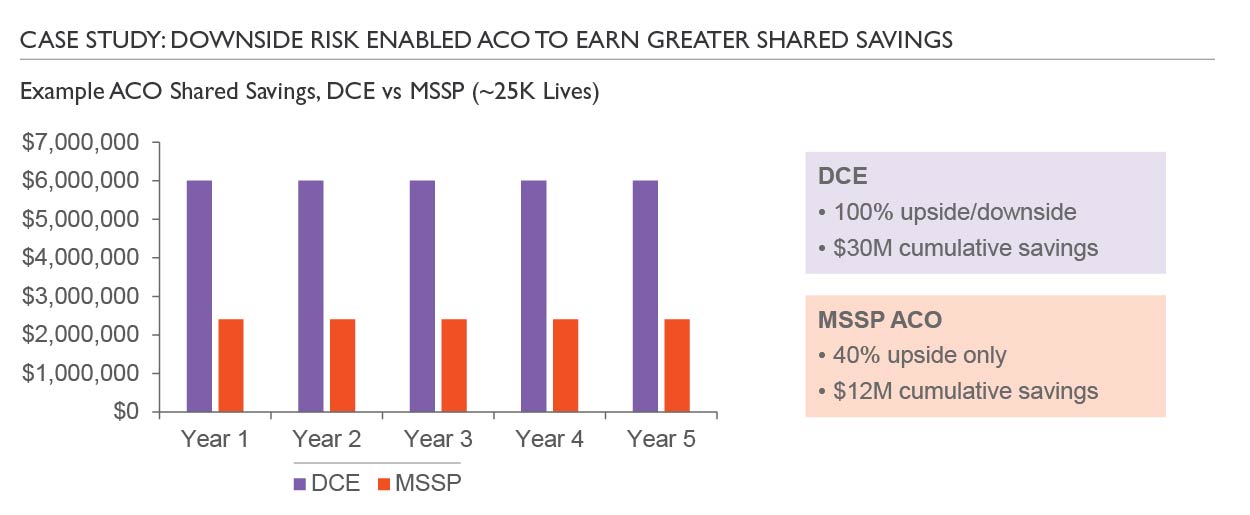
This analysis highlights why many new entrants into VBC (e.g., ChenMed, agilon, Oak Street Health, Iora Health, etc.) optimize contracting strategy for upside potential. For all of the clinical work that can create value, downside risk is usually essential for maximizing the value capture. Additionally, downside risk drives organizational accountability and focus in a way that upside-only models have been unable to deliver. That said, organizations should always be strategic about when, where and how to take on downside risk.
Key takeaways:
- Provider organizations benefit from a more nuanced approach to risk and the mechanisms for managing it
- Understanding the differences between actuarial and performance risk can help organizations position their contracts and overall approach to VBC accordingly
- Establishing and maintaining reasonable baseline targets is important to avoid the proverbial ‘race to the bottom’
- Downside risk can be a powerful strategic lever for increasing upside opportunity
- Downside financial accountability can drive organizational focus on VBC
No matter where your organization stands today on its journey to value-based care, our value-based care experts are equipped to provide your organization with unique insights and impactful recommendations in prioritizing opportunities and positioning your organization for select value-based care undertakings. Reach out to us for more information or to speak with an Sg2 value-based care expert.
Related resources:
- Share




